

INTRODUCTION
Spindle cell lipoma (SCL) is an uncommon benign subcutaneous adipose tissue tumor. They most commonly appear as a slow-growing and painless mass at the shawl region (shoulder, posterior neck, and upper back) of middle-aged men (10:1 male-to-female ratio) at an average size of 4-5 cm [1,2]. Because the histological finding is similar to malignant lipomatous tumors such as liposarcoma, a precise diagnosis of SCL is essential, especially when they appear as larger masses. We present a rare case of a huge-sized occipital and upper posterior neck SCL successfully removed through local excision.
Ethical statements
This study was approved by the Institutional Review Board (IRB) of the Ewha Womans University Mokdong Hospital (IRB no: EUMC 2023-02-021). Written informed consent was obtained from the patient to publish this case report. A copy of the written consent is available for review on request.
CASE REPORT
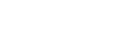
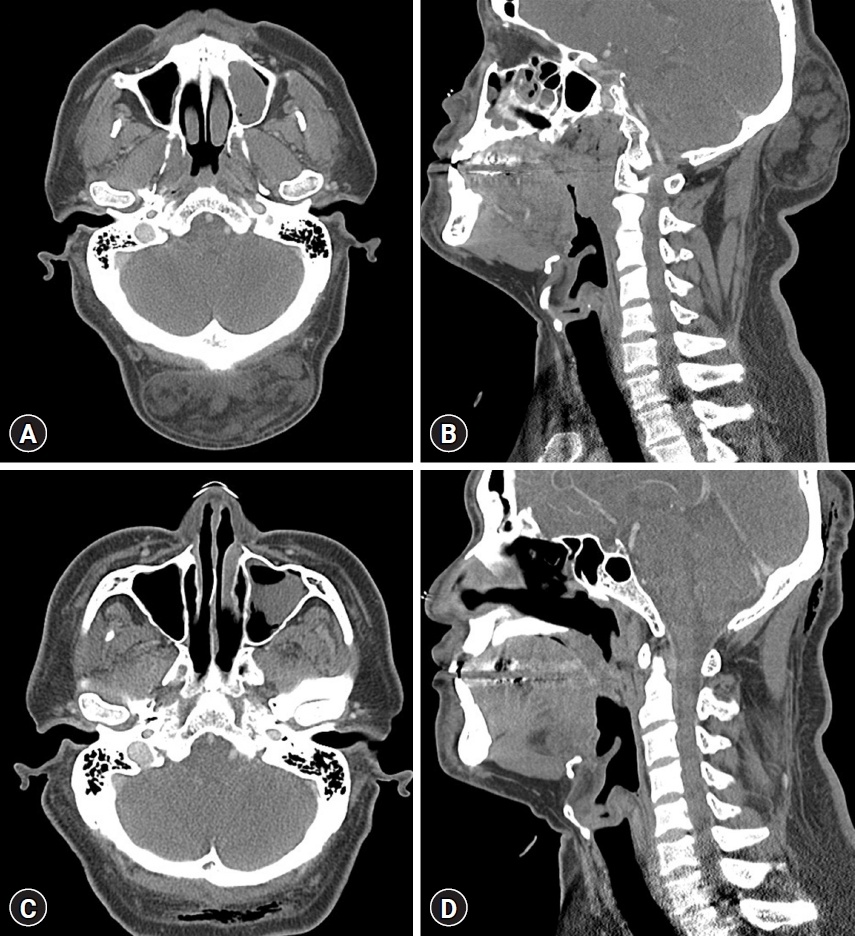
A 49-year-old man complained of a mass in the occipital area that had slowly grown in size for 4 years (Fig. 1). He had no history of trauma or surgery in the area, and except for diabetes mellitus, he had no other medical history or allergy. On physical examination, we could check a huge palpable and movable mass that was elastic and soft. There was no tenderness, redness, or heating sensation on the mass. Computed tomography of his neck revealed a 10-×9.5-cm-sized, well-circumscribed, non-enhancing solid and fatty mass in the occipital area/posterior neck (Fig. 2).
The patient underwent surgical excision of the tumor under local anesthesia, located between the subcutaneous tissue and occipital bone/posterior neck muscles. It was well encapsulated and dissected from the adjacent tissue. There were no adhesions to adjacent tissues or vascular involvement. Until it was completely excised, including the tumor capsule, the sharp dissection was done around the lesion. The dead space was closed beneath the skin using buried, interrupted 2-0 vicryl sutures. The mass was 10×9.5×5 cm and was removed entirely without complications (Fig. 3). The patient was followed up in the outpatient department 2 weeks postoperatively with an unremarkable physical exam, with the wound completely healed without swelling or redness.
On histological examination, H&E stained sections showed the lesion consists of mature adipose tissue, bland spindle cells, and ropey collagen with myxoid stroma (Fig. 4A). Immunostaining showed spindle cells for CD34-positive (Fig. 4B), S100 protein-negative, retinoblastoma 1 (Rb1) absent, and alpha-smooth muscle actin-negative. Based on these findings, a histopathological diagnosis of SCL was given. There was no recurrence 1 year after the surgery.
DISCUSSION
Lipomas are slow-growing, benign adipose tumors mainly occurring in the subcutaneous tissues of the head and neck [3]. Usually, lipomas are asymptomatic, can be detected incidentally, and do not need treatment. SCL is an uncommon benign histopathological variant of lipoma that Enzinger and Harvey [1] first described in 1975 based on its characteristic histological findings characterized by collagen-rich spindle cells taking over adipocytes. SCL commonly occurs between 40 and 60 years old, are more prevalent in males [2]. Most SCL involves subcutaneous tissue of the upper back, shoulders, and posterior neck [4]. In rare cases, these tumors occur in other sites, including the face, oral cavity, and extremities [5]. In a study of 395 SCL patients, Ko et al. [2] reported that 331 (86%) occurred in men; 53 (14%) in women. SCL in women frequently occurs outside the shawl region compared with men and at a slightly younger patient age than men (median age 51 years vs. 64 years).
Grossly, SCL is a well-circumscribed, oval mass in the subcutaneous tissue and has a yellow-tan cut surface with grey-white and myxoid foci [6]. The texture is similar to typical lipomas, although it may be somewhat firmer, especially if the spindle-cell component is more dominant. Microscopically, SCL is characterized by mature adipocytes, bland spindle cells in parallel bundles, and hyalinized rope-like collagen fibers (ropy collagen) [6]. On immunohistochemistry, the spindle cells exhibit CD34, and they are negative for S100 protein. Loss of nuclear Rb1 protein expression is also a characteristic finding. On the other hand, liposarcoma, which must be differentiated from SCL, is essentially CD34-negative and S100-positive [6,7]. Both SCL and pleomorphic lipomas exhibit losses of chromosomes 13q and/or 16q-losses considered characteristic for this family of lipomas [8]. As mentioned above, most SCLs are composed of varying proportions of adipose tissue and spindle cells, which can lead to a variety of imaging findings, and it is very rare for either to be predominant. Therefore, the diagnosis of spindle-cell lipoma should be considered when one encounters a well-defined, heterogenous, fatty mass in the subcutis of a middle-aged man, especially when the mass is localized to the posterior neck [9].
Total excision, including tumor capsule, is considered as the primary treatment for SCL. In a recent study, Chen et al. [10] reported that none of the 40 patients with SCL recurred during follow-up for 2 to 105 months after surgery.
CONCLUSION
We present an unusual case of a huge-sized SCL on the occipital area and the upper posterior neck. Because of histological similarities, clinicians must confirm immunochemical findings when encountering spindle cell-associated soft tissue tumors to avoid misdiagnosis after total excision.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






